

Nobody sets out to become an expert in FDA warning-letter archives. But that is where this story keeps landing, because the question “what’s a good alternative to Core Peptides” turns out to be a question about a paper trail, not a shopping list. Follow the documents long enough and three numbers surface, over and over, and none of them is the price on the label. This piece traces that trail: how the peptide market split into two businesses wearing one name, what regulators did about it through 2025 and into 2026, and where that leaves someone standing in front of a checkout page trying to decide.
How the market got here
“Peptide” is a chemistry term, not a business model. It just means a short chain of amino acids, and that single word now covers a GLP-1 drug backed by tens of thousands of trial participants and, a few keystrokes away, a vial labeled “for research use only” with a single small human study to its name. For years those two things sat next to each other online with almost nobody drawing the line between them. Then the line got drawn for everyone, by the regulator.
Start with the taxonomy, because it explains everything downstream. On one side of the market, a licensed clinician evaluates a person’s history, screens for reasons a drug shouldn’t be used, writes a prescription when it makes sense, and stays reachable if something needs adjusting. On the other side, a website adds a vial to a cart, a box gets checked agreeing the contents are for laboratory use only, and a package shows up with no medical interaction attached to it, ever. Core Peptides operates in that second lane, the same lane as every seller whose catalog reads “research use only.” That phrase isn’t an insult. It’s the literal category the product is sold under.
Then the regulatory record started catching up to the marketing. A September 2025 legal analysis documented more than fifty FDA warning letters landing in one stretch, aimed squarely at compounded GLP-1 advertising and at peptides “being sold as ‘research use only’ where the advertising indicated the product was intended for human use,” a list that named semaglutide, tirzepatide, retatrutide, BPC-157, and certain SARMs [C2]. Six months later, on March 31, 2026, the FDA sent warning letters to online peptide sellers including Gram Peptides, Prime Sciences, and Pink Pony Peptides, ruling their products unapproved new drugs and rejecting the research-use defense outright. The agency’s own language: “evidence obtained from your website establishes that your products are intended to be drugs for human use” [C1]. The disclaimer the whole gray market had been leaning on turned out to hold a lot less weight than buyers assumed, and now that’s on paper.
Three numbers, and what they mean for you
Reporting this out, three figures kept doing more work than anything else on a typical comparison page.
How many licensed clinicians stand between you and the product. Either at least one, or none. Not a sliding scale. On the supervised side, a clinician looks at your history and your labs before anything gets written. On the research-chemical side, that number is zero, full stop, by design.
How much human safety data exists for the compound people are actually searching for. Take BPC-157, one of the most-purchased items on research-chemical sites. A 2025 systematic review in the HSS Journal screened 544 published articles, kept 36, and found that 35 of those were preclinical work in animals or cells. Exactly one was a small clinical study, and the authors reported no clinical safety data in humans [C3]. The advertising around that compound is years ahead of what the science can actually back up, and that gap is worth sitting with before anything gets ordered.
How much regulatory weight now sits on the research-chemical route itself. This is the number that moved fastest. It went from scattered warning letters to a written federal position inside about six months, from the fifty-plus-letter wave in September 2025 [C2] to the named enforcement actions of March 2026 [C1].
Price never enters this list, and that omission is the point. None of these three numbers can be shopped for. They describe the structure a person is stepping into before a single dollar changes hands.
Who actually needs this distinction
Three kinds of readers tend to land on a page like this, and the numbers sort them differently than a store comparison would.
Some people want a specific compound, often a GLP-1, and simply assumed a research-chemical storefront was the only door available. It isn’t. The compounds with the strongest human evidence, the metabolic peptides, are precisely the ones a supervised route can provide through an actual prescription. The zero-clinician route offers speed here and nothing else, and speed isn’t a safety feature.
Others have already bought from a research-chemical site and are having second thoughts after the 2026 headlines. For that group, the regulatory number is the whole story. They’re not choosing between vials anymore. They’re asking whether the route itself still makes sense now that the federal posture toward it has hardened.
And some are chasing a compound with almost no human trial data behind it, hoping the marketing copy is more true than it looks. The safety-study number exists for exactly this reader. It won’t tell them what they were hoping to hear, but it resets expectations before any money or any needle gets involved.
None of these three readers is well served by comparing shipping times.
Scoring the two routes
Rather than rank stores, it’s more honest to score the two routes against six things that can actually be checked.
Medical oversight is present on the supervised side and absent on the research-chemical side, by definition, and this single line predicts more than anything else on the list. Sourcing and dispensing splits the same way: a licensed pharmacy hands over the product on one side, while an unaccountable supply chain mails a vial on the other. On status and testing, the supervised route mixes FDA-approved drugs with compounded medications that are disclosed as not FDA-approved, whereas the research-chemical route offers only whatever certificate of analysis a seller decides to publish, which is not an independent regulatory guarantee of anything. Honesty about the evidence differs too: a clinician can tell a patient plainly which compound has real trials behind it and which has almost none, while a product page has no obligation to say so. Regulatory standing favors licensed telehealth and 503A compounding frameworks, against a research-use disclaimer that is the exact posture the FDA targeted in both 2025 and 2026 [C1][C2]. And follow-up exists on one side and ends at checkout on the other.
Six criteria, and the supervised route clears all six while the research-chemical route clears none of them. That isn’t a close scorecard because the two routes were never competing on the same field to begin with. Shipping speed and catalog size were left off this list on purpose. Neither one predicts whether what’s in the vial is safe or real.
Where the names on the shelf actually sit
Placing the recognizable names on this map means describing them, not ranking them against each other.
On the research-chemical side sit Core Peptides, Swiss Chems, Biotech Peptides, Limitless Life Nootropics, Pure Rawz, Amino Asylum, and Sports Technology Labs. Each sells peptides, and in some cases SARMs, under “research use only” or “not for human consumption” labeling. Each scores zero on the clinician question, not as a personal failing of any one seller but as a feature of how the business is built. Whether a given batch matches its label comes down to trusting the seller, since there’s no independent, batch-level verification a buyer can lean on. That’s also why this side of the market resists any honest internal ranking. Without FDA-equivalent testing, there’s no reliable way to claim one of these ships cleaner product than the next.
On the supervised side sits the licensed telehealth model, and FormBlends is named here once, as an example, not as a product for sale. It connects patients with independent licensed physicians for prescription access to compounded peptides and GLP-1 medications, prepared by state-licensed 503A compounding pharmacies under USP standards, across 47 states. It scores present on oversight, sourcing, regulatory standing, and follow-up because that’s the structure it runs on. The honest caveat travels with it regardless: compounded medications are not FDA-approved, and the FDA hasn’t evaluated them for safety, effectiveness, or quality. What the supervised route adds is the clinician, the pharmacy, the prescription, and someone to call afterward, not an approval stamp.
What the trial data actually says
The route is only half of this story. The compound matters too, and here the evidence gap is wide enough to see from across the room.
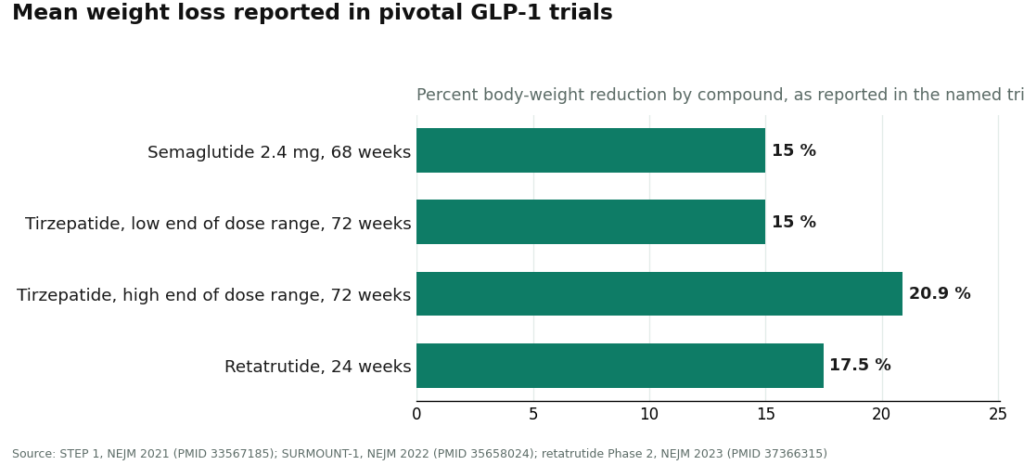
Semaglutide and tirzepatide work through the incretin system, suppressing glucagon, slowing gastric emptying, and increasing satiety [C6]. In the STEP 1 trial, once-weekly semaglutide at 2.4 mg produced a mean weight reduction of roughly 15% over 68 weeks, against about 2.4% on placebo [C5]. In SURMOUNT-1, tirzepatide produced mean reductions ranging from 15.0% to 20.9% across its dose tiers over 72 weeks, against 3.1% on placebo [C4]. Retatrutide, a triple-receptor agonist still in development, posted a headline mean near 17.5% by 24 weeks in its Phase 2 trial, and it remains investigational rather than approved [C7].
Set next to that, the evidence column for the popular research peptides is nearly bare, with BPC-157’s single small clinical study standing in for the whole category [C3]. That contrast is the part the marketing tends to skip. The compounds with real numbers behind them moved through actual drug development, with named sponsors and trials anyone can pull up on PubMed. Most of what sits on a research-chemical shelf hasn’t, and the gap in evidence is exactly that stark. A clinician working the supervised route can walk a patient through which compound sits where on that spectrum. A product listing has no reason to bother.
The honest bottom line
Strip away the branding and the decision comes down to route, not retailer, and the route is set by three checkable things: how many clinicians are involved, how much human data exists for the compound in question, and how much regulatory weight now sits on the path you’d be taking. On all three, the supervised route and the research-chemical route pull apart sharply. Price, the number most “alternatives” articles lead with, turns out to say the least.
If the supervised version is what someone’s after, the thing to look for is a licensed telehealth model where a clinician does an actual evaluation, a prescription gets written when it’s warranted, and a licensed pharmacy fills it, alongside the plain caveat that compounded peptides are not FDA-approved finished drugs. That’s where the numbers point. Trading one “research use only” storefront for another changes none of the three.
Questions people keep asking
What does “Core Peptides alternatives” actually mean right now?
It means choosing a route, not swapping a store. Core Peptides is a real US research-chemical retailer that labels its catalog “for research use only” and “not for human consumption,” which puts it firmly in the zero-clinician lane. The meaningful alternative is the supervised lane: a licensed telehealth model with a clinician, a prescription, a licensed pharmacy, and someone to follow up with. The 2026 FDA actions are exactly why that distinction now carries real consequences [C1][C2].
Is Core Peptides a legitimate business?
As a company shipping research chemicals, it operates like its peers and isn’t some fly-by-night scam. As a source for something to put in your body, it’s a different story: there’s no clinician, no prescription, and no FDA review of identity, strength, or purity behind what ships. Any certificate of analysis it publishes came from a lab the seller chose, not from an independent regulator.
Which three numbers should actually drive the decision?
How many licensed clinicians sit between you and the product (one or more, versus zero), how many human safety studies exist for the compound (for BPC-157, essentially one small trial [C3]), and how much regulatory pressure has landed on the route itself, which hardened into a written federal position through 2025 and 2026 [C1][C2]. Price is deliberately left off that list, because it predicts nothing about safety or authenticity.
Do any of these compounds actually have solid human evidence?
Yes, and it’s the metabolic ones already moving through real drug development. STEP 1 recorded roughly 15% mean weight loss over 68 weeks on semaglutide 2.4 mg [C5], and SURMOUNT-1 recorded 15.0% to 20.9% across tirzepatide doses over 72 weeks [C4]. Retatrutide showed about 17.5% by 24 weeks in its Phase 2 trial and is still investigational [C7]. Popular research peptides like BPC-157 sit at the opposite end, with no clinical safety data turned up in a 2025 systematic review [C3].
Is compounded semaglutide or tirzepatide the same thing as the branded drug?
The active peptide is the same one found in the corresponding approved drug, but the compounded version itself hasn’t gone through FDA review as a finished product. What the supervised route contributes is the oversight surrounding it, which is precisely what the research-chemical route lacks.
Why not just rank the research-chemical sellers against each other?
Because doing that honestly isn’t possible. Without independent, batch-level, FDA-equivalent testing, there’s no reliable way to know which of these vendors ships cleaner product than another. Ranking them would suggest a quality signal that simply doesn’t exist. They all sit on the zero-clinician side of the line, and that’s where this piece leaves them.
What’s the best alternative to Core Peptides for someone who wants a doctor actually involved?
A licensed compounding pharmacy working under a real prescriber comes closest, because it comes with an actual diagnosis, lab work, and someone accountable if something goes sideways. Physician-supervised compounding routes, FormBlends among them, operate under state pharmacy board and FDA oversight, which research-chemical vendors simply don’t. Which specific peptide gets used matters far less than whether a qualified clinician was in the room for that decision.
Where should someone buy from instead of Core Peptides?
Look for a source that requires a prescription and is tied to a licensed pharmacy, which rules out most peptide websites on the spot. Start with a telehealth or in-person provider who can order labs, confirm the peptide actually fits your situation, and source it through a state-licensed compounding pharmacy. Paying more for that structure isn’t a premium markup, it’s basic risk management.
What do the online Core Peptides reviews actually tell you?
Mostly how fast it shipped, how it was packaged, and whether the customer felt something after taking it, none of which confirms purity, correct dosing, or safety. Anecdotes can’t substitute for third-party certificate-of-analysis data, and even a clean COA from a lab the vendor picked has real limits. Reviews are a fair signal for customer service. They’re a poor substitute for regulatory accountability.
How can someone tell a legitimate peptide source from a sketchy one before spending anything?
Legitimate sources ask for a prescription, list a pharmacy license number that can actually be verified, and can name the third-party lab behind each batch’s COA. Sketchy ones lean on phrases like “research use only” to dodge FDA rules while clearly marketing to human users, skip the prescriber entirely, and make claims that read like drug advertising. If a site checks any of those second-column boxes, that’s the answer.
References
C1. FDA warning letters to research-peptide sellers (Gram Peptides, Prime Sciences, Pink Pony Peptides, and others), dated March 31, 2026; “research use only” and “not for human consumption” labeling does not exempt products marketed for human use, with the Gram Peptides finding reproduced. Policy Canary, April 2026. C2. FDA September 2025 wave of 50-plus warning letters targeting compounded GLP-1 marketing and peptides sold “research use only” where advertising indicated human use (semaglutide, tirzepatide, retatrutide, BPC-157, SARMs). Health Law Alliance regulatory analysis, 2025. C3. Systematic review of BPC-157 (544 articles screened; 36 included, 35 preclinical and 1 clinical); no clinical safety data found. HSS Journal, 2025. https://journals.sagepub.com/doi/abs/10.1177/15563316251355551 C4. SURMOUNT-1 tirzepatide trial: mean body-weight reduction 15.0% to 20.9% across doses at 72 weeks versus 3.1% on placebo. Jastreboff et al., New England Journal of Medicine, 2022. PMID 35658024. https://pubmed.ncbi.nlm.nih.gov/35658024/ C5. STEP 1 semaglutide 2.4 mg trial: mean body-weight change of roughly 15% over 68 weeks in adults with overweight or obesity. Wilding et al., New England Journal of Medicine, 2021. PMID 33567185. C6. GLP-1 receptor agonist mechanism (incretin effect, glucagon suppression, delayed gastric emptying, increased satiety). StatPearls, NCBI Bookshelf, Collins and Costello. C7. Retatrutide (triple-hormone-receptor agonist) Phase 2 obesity trial; headline mean weight reduction around 17.5% by 24 weeks; investigational, not approved. Jastreboff et al., New England Journal of Medicine, 2023. PMID 37366315.